What is mesothelioma?
Malignant mesothelioma is a rare cancer that occurs in the thin layer of tissue that covers the majority of your internal organs (mesothelium).
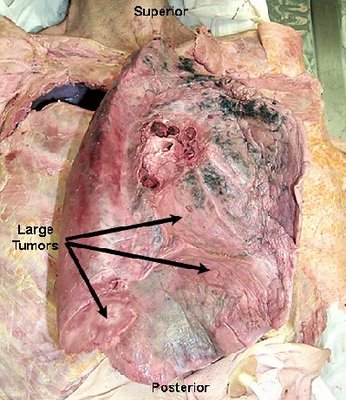
Doctors divide mesothelioma into different types based on what part of the mesothelium is affected. Mesothelioma most often affects the tissue that surrounds the lungs (pleura). This type is called pleural malignant mesothelioma. Other, rarer types of mesothelioma affect tissue in the abdomen, around the heart and around the testicles.
Mesothelioma is an aggressive and deadly form of cancer. Mesothelioma treatments are available, but for many people with mesothelioma, a cure is not possible. Instead, treatment for mesothelioma is often focused on keeping you as comfortable as possible.
Signs and symptoms of mesothelioma vary depending on where the cancer occurs.
Pleural mesothelioma, which affects the tissue that surrounds the lungs, causes signs and symptoms that may include; Chest pain under the rib cage, Painful coughing, Shortness of breath, Unusual lumps of tissue under the skin on your chest, Unexplained weight loss, Peritoneal mesothelioma, which occurs in tissue in the abdomen, causes signs and symptoms that may include:
Abdominal pain, Abdominal swelling, Lumps of tissue in the abdomen, Unexplained weight loss
Different forms of mesothelioma
Signs and symptoms of other types of mesothelioma are unclear. Other forms of mesothelioma are so rare that not much information is available. Pericardial mesothelioma, which affects tissue that surrounds the heart, can cause signs and symptoms such as breathing difficulty and chest pains. Mesothelioma of tunica vaginalis, which affects tissue surrounding the testicles, may be first detected as a mass on a testicle.
Check with your doctor
See your doctor if you have signs and symptoms that may indicate mesothelioma. Signs and symptoms of mesothelioma aren't specific to this disease and, due to the rarity of mesothelioma, are more likely to be related to other conditions. If any persistent signs and symptoms seem unusual or bothersome to you, ask your doctor to evaluate them.
Causes of Mesothelioma
In general, cancer begins when a series of genetic mutations occur within a cell, causing the cell to grow and multiply out of control. It isn't clear what causes the initial genetic mutations that lead to mesothelioma, though researchers have identified factors that may increase the risk. It's likely that cancers form because of an interaction between many factors, such as inherited conditions, your environment, your health conditions and your lifestyle choices.
Mesothelioma doesn't include a noncancerous tumor. A form of noncancerous (benign) tumor that can occur in the chest is sometimes called benign mesothelioma. However, this name is misleading. Benign mesothelioma doesn't begin in the same cells where the cancerous forms of mesothelioma begin. And, in a minority of cases, benign mesothelioma can be very aggressive, despite the term "benign." For this reason, some doctors now refer to this tumor as solitary fibrous tumor.
Solitary fibrous tumor usually doesn't cause signs and symptoms. Most cases are inadvertently discovered during tests and procedures for other conditions. It isn't clear what causes solitary fibrous tumors, but they aren't linked to asbestos exposure. Treatment for solitary fibrous tumor typically includes surgery.
Asbestos exposure: The primary risk factor for mesothelioma
Asbestos is a mineral that's found naturally in the environment. Asbestos fibers are strong and resistant to heat, making them useful in a wide variety of applications, such as in insulation, brakes, shingles, flooring and many other products.
When asbestos is broken up, such as during the mining process or when removing asbestos insulation, dust may be created. If the dust is inhaled or swallowed, the asbestos fibers will settle in the lungs or in the stomach, where they can cause irritation that may lead to mesothelioma, though how exactly this happens isn't understood. It can take 20 to 40 years or more for mesothelioma to develop as a result of asbestos exposure.
Some people with years of asbestos exposure never develop mesothelioma. And yet, others with very brief exposure develop the disease. This indicates that other factors may be involved in determining whether someone gets mesothelioma or doesn't. For instance, you could inherit a predisposition to cancer or some other condition could increase your risk.
Possible risk factors
Factors that may increase the risk of mesothelioma include:
Personal history of asbestos exposure. If you've been directly exposed to asbestos fibers at work or at home, your risk of mesothelioma is greatly increased.
Living with someone who works with asbestos. People who are exposed to asbestos may carry the fibers home on their skin and clothing. These stray fibers can put others in the home at risk of mesothelioma. People who work with asbestos should shower and change clothes before leaving work.
A monkey virus used in polio vaccines. Some research indicates a link between mesothelioma and simian virus 40 (SV40), a virus originally found in monkeys. Millions of people may have been exposed to SV40 when receiving polio vaccinations between 1955 and 1963, because the vaccine was developed using monkey cells. Once it was discovered that SV40 was linked to certain cancers, the virus was removed from the polio vaccine. Whether SV40 increases the risk of mesothelioma is a point of debate, and more research is needed.
Radiation. Some research links mesothelioma to the radioactive substance thorium dioxide, which was used along with X-rays to diagnose various health conditions from the 1920s to the 1950s. Mesothelioma has also been linked to radiation therapy treatments to the chest, such as those used to treat breast cancer or lymphoma.
Family history. A family history of mesothelioma may increase your risk of mesothelioma, but more research is needed to understand this theory.
Mesothelioma Complications
As pleural mesothelioma spreads in the chest, it puts pressure on the structures in that area. This can cause complications, such as:
- Difficulty breathing, Chest pain, Difficulty swallowing,
- Swelling of the neck and face caused by pressure on the large vein that leads from your upper body to your heart (superior vena cava syndrome)
- Pain caused by pressure on the nerves and spinal cord, Accumulation of fluid in the chest (pleural effusion), which can compress the lung nearby and make breathing difficult
Prevention
Reducing your exposure to asbestos may lower your risk of mesothelioma.
Find out whether you work with asbestos environment
Most people with mesothelioma were exposed to the asbestos fibers at work. Workers who may encounter asbestos fibers include:
- Miners, Factory workers, Insulation manufacturers, Ship builders, Construction workers, Auto mechanics
Ask your employer whether you have a risk of asbestos exposure on the job.
Follow your employer's safety regulations
Follow all safety precautions in your workplace, such as wearing protective equipment. You may also be required to shower and change out of your work clothes before taking a lunch break or going home. Talk to your doctor about other precautions you can take to protect yourself from asbestos exposure.
Be safe around asbestos in your home
Older homes and buildings may contain asbestos. In many cases, it's more dangerous to remove the asbestos than it is to leave it intact. Breaking up asbestos may cause fibers to become airborne, where they can be inhaled. Consult experts trained to detect asbestos in your home. These experts may test the air in your home to determine whether the asbestos is a risk to your health. Don't attempt to remove asbestos from your home — hire a qualified expert. The Environmental Protection Agency offers advice on its website for dealing with asbestos in the home.